
Do you struggle with carpal tunnel, poor dream recall, low motivation, anxiety (especially social anxiety), weird reactions to magnesium and glutamine, or histamine and/or oxalate issues?
I can help! I think I’ve cracked the code here. 🙂
There could be a few reasons behind these strange symptoms, but a common one is deficiency in one of the B vitamins – specifically, B6!
B6 is responsible for some 140 different processes in the body! It helps us make neurotransmitters like serotonin, which is responsible for our mood, and plays an important role in gut health as well.
Supplementing can help with carpal tunnel, mood, gut health, and even other things like sleep, stress, food sensitivities (glutamate, oxalates, histamines), and mood-related symptoms (depression, anxiety, motivation, etc.).
In some cases, people can have a B6 + zinc deficiency together, known as pyroluria, that can cause additional symptoms, especially those related to mood (and this may even be the cause of introversion)!
But before you rush out and buy B6, please note that some people may have adverse reactions to taking it… I often recommend starting with the pyridoxal 5′-phosphate version, also known as P5P.
In this article, you will learn about:
- The importance of vitamin B6 in the body
- B6 deficiencies in Hashimoto’s: causes and symptoms
- A co-occurring B6 and zinc deficiency (pyroluria)
- Root cause treatment protocols
- B6 toxicity precautions and choosing supplements
B6 in the Body and Brain
Vitamin B6 is one of the eight B vitamins. It’s a water-soluble vitamin found in three forms: pyridoxine hydrochloride, pyridoxal, and pyridoxamine. For vitamins to be used by the body, they must first be converted. In this case, all of these must be converted into activated pyridoxal-5-phosphate (P5P) by the liver.
P5P is the form of vitamin B6 the body requires for a range of actions. It is a cofactor (a molecule that helps enzymes function) which supports over 140 enzymatic reactions throughout the body. For example, B6 helps to produce gamma-aminobutyric acid (GABA), an important mood-related neurotransmitter. Vitamin B6 is also needed for glucose production, as well as amino acid and lipid metabolism. [1]
It helps with the metabolism of certain foods which may build up and become toxic, such as glutamates, oxalates, and histamines. [2]
Because of its role in producing neurotransmitters, a P5P (vitamin B6) deficiency (even a mild deficiency) can contribute to low serotonin and dopamine levels. Other symptoms that people may experience with low B6 levels include carpal tunnel, sleep issues, mood changes, changes in cardiovascular function, and a loss of hormone secretion. [3]
Here is a summary of the essential roles that B6/P5P plays in the body:
- Breaks down proteins into amino acids that convert to important mood-related neurotransmitters (chemical messengers of the nervous system)
- Breaks down foods like proteins, fats and carbohydrates, as well as food components which may build up and become toxic
- Aids with digestion, gut motility, and detoxification (may aid in resolving gut issues like constipation and SIBO)
- Contributes to healthy immune function
- Helps maintain normal levels of homocysteine (an inflammatory marker)
- Creates hemoglobin, the part of red blood cells that carries oxygen
- Breaks down histamines, glutamates and oxalates, which are common problematic food components
- Some research suggests that P5P may have a cardioprotective effect [4]
Vitamin B6 is found in high amounts in whole food sources like chickpeas, beef liver, tuna, salmon, and chicken. However, even if someone is getting enough B6 through their diet, they may still have a hard time converting B6 into the active form of P5P, which can lead to a deficiency. Furthermore, I’ve come to realize that many of the B vitamins provide benefits at mega doses through receptor binding, beyond the RDA, so I often find that supplements move the needle when food interventions don’t.
Since the human body cannot store B6, a daily source is required. The nutrient is taken into the body from the protein in our diet, and is also synthesized internally by specific bacteria in the gut.
*Note: Through this article, we may use the terms “B6” and “P5P” interchangeably for general discussion purposes. However, they are not exactly the same. P5P, the active form of B6, is the supplement that I recommend for people with deficiencies, in order to prevent a buildup of pyridoxine.
B6 and Neurotransmitter Production
P5P converts the amino acid glutamine into the neurotransmitter GABA, which promotes feelings of calm. It also helps our brains produce serotonin, the “feel good” neurotransmitter. [5] In the case of B6 deficiency, glutamate, an excitatory neurotransmitter, may be produced from glutamine and glycine. This is why some people experience paradoxical reactions of feeling worse with taking magnesium glycinate, glutamine and glycine. They may also feel more anxious, edgy and restless after taking one of the above mentioned supplements which are supposed to produce a relaxing effect (more about that below).
Dopamine, another mood-related hormone, is also produced with the help of P5P. Dopamine helps with our motivation, focus, and feelings of pleasure and reward (alcohol and recreational drugs target dopamine receptors as well).
P5P also affects the production of melatonin, the sleep hormone. [6] As such, it plays a role in sleep and mood, as well as in other functions, including appetite. Because of the way it affects the production of neurotransmitters, taking P5P as a supplement may promote mental well-being and reduce feelings of depression, anxiety, and stress. [7]
Additionally, B6 is a cofactor in producing serotonin, the neurotransmitter that’s helpful for happiness, lowered anxiety, and proper gut motility. Some people supplement with the amino acid and popular supplement 5-HTP to address depression, but adequate levels of P5P are actually required to convert 5-HTP to serotonin. So, if you want to supplement with 5-HTP, you should also be supplementing with P5P.
B6 and Gut Motility
We used to think that serotonin was primarily produced and used in the brain and nervous system, but researchers now know that around 95 percent of the neurotransmitter serotonin is produced in the gut! [8]
Serotonin plays an important role in digestion. Because of its role in serotonin production, P5P levels influence digestive functioning, particularly gut motility, or the ability for the gut to process food properly, as well as how sensitive your intestines are to sensations like pain and fullness from eating. [9]
B6 deficiencies have been associated with a greater incidence of a variety of functional intestinal disorders, and can contribute to slowed gastrointestinal (GI) motility (the slowed passage of food through the digestive system). Lack of motility is one of the main root causes of both constipation and small intestinal bacterial overgrowth (SIBO), as when the passage of food slows down in the GI tract, it gives bacteria time to “set up shop” and colonize the small intestine. [10]
One study found that low B6 intake was associated with irritable bowel syndrome (IBS) symptoms, and people with IBS and constipation had low levels of serotonin. Targeting serotonin receptors is one potential intervention that has been used in the treatment of IBS. [11]
B6 can be acquired from our diet and is also produced in the gut by specific bacteria, so our gut health plays an important role in vitamin B6 levels. There are six bacterial species that can synthesize B6. [12]
B6 and Immune Health
Low levels of B6 (P5P) have been linked to chronic inflammation. Numerous studies have found deficiencies may influence gut inflammation, gut infections, allergies, degraded immune response, neuro-inflammatory diseases, and reductions in the cytotoxic activity of natural killer cells which defend against viral infections and cancer. [13]
Animal studies have found that supplementing with vitamin B6 reduced the number of tumors in the colon. They have also shown that low levels may be a potential risk factor for colorectal cancer and other conditions of chronic inflammation, including cardiovascular disease. [14]
Homocysteine Regulation
Homocysteine is an important amino acid in the blood, which B6 (as well as B12 and folate) help to break down. High levels of homocysteine have been linked with inflammation in the body, which can be due to deficiencies in B6, B12, and/or folate. [15]
When homocysteine builds up, this can inhibit methylation, one of the body’s key detoxification processes. The homocysteine overload can result in cell damage, including mitochondrial membrane damage and DNA strand breakage.
Elevated levels of homocysteine have been associated with pregnancy complications, [16] cardiovascular disease, [17] inflammatory bowel disease, as well as a number of other conditions. [18]
Homocysteine builds up during periods of chronic stress — there is a significant relationship, for example, between chronic job-related stress and plasma homocysteine levels. We know that stress is a common trigger in Hashimoto’s, as well as a cause for reduced levels of B6 in the body. [19]
I have found that poor methylation is common in Hashimoto’s, and that many people in our community have the MTHFR gene variation, which further impacts methylation and results in elevated levels of homocysteine (making B6 deficiency even more impactful).
Metabolism of Glutamates, Oxalates, and Histamines
B6 helps us both tolerate and break down food components that are often problematic for those with Hashimoto’s — the key three being glutamates, oxalates, and histamines. This is why B6 (P5P) is one of the first things I recommend to support gut health.
P5P promotes the tolerance of various foods that may cause sensitivity or intolerance, including foods that contain histamines [20] (vitamin B6 is a cofactor in breaking down histamines), oxalates [21] (correcting a B6 deficiency can help with symptoms of oxalate buildup), and glutamates (studies show that supplementing with B6 may help with neurological reactions to glutamate). [22]
Glutamate, Glutamine, Bone Broth, Glycine, and Magnesium Glycinate Reactions
Glutamate acts as an excitatory neurotransmitter, overstimulating brain cells, and too much can lead to headaches, anxiety, and insomnia. Glutamate is found in many foods such as processed meats, some cheeses, Asian sauces, and nuts (monosodium glutamate or MSG is an example of a common source of glutamate).
One interesting study found that the headache reaction some people get (this is called MSG Symptom Complex, but was once referred to as “Chinese Restaurant Syndrome”) after eating foods with MSG, correlated to their having a low level of vitamin B6. In these same individuals, symptoms did not reoccur once treated with B6 supplementation. [23] Other research has found that leaky gut (common in Hashimoto’s) can increase the level of glutamate that enters the central nervous system. [24]
Some individuals also can over-convert glutamine, glycine, and magnesium glycinate into glutamate when they have a B6 deficiency, and this may lead them to have symptoms like agitation, irritability and insomnia. (This can also happen with L-glutamine-rich foods, such as bone broth.)
Oxalates
Preliminary research has also linked the build-up of oxalates to thyroid disease, [25] and I have noticed that some people with Hashimoto’s do indeed report symptoms like joint pain, burning with urination, interstitial cystitis, leaky gut, depression, and kidney stones when eating high-oxalate foods such beets, chard and celery.
Beyond foods, having an overgrowth of yeast or mold in the body can lead to the internal production of oxalates, causing the same symptoms.
B6 is a cofactor for the breakdown of oxalates, and after doing hundreds of Organic Acid Tests, I’ve noticed that B6 deficiency can lead to a build up of oxalates. In my experience, supplementing with B6 can lower oxalate levels though increased metabolism. [26]
Beyond foods and fungus, please note that an intake of glutamine, glycine, and magnesium glycinate may also lead to an overproduction of oxalates via the glyoxylate pathway.
The glyoxylate pathway is related to the citric acid cycle (CAC), where glyoxylate is produced in the liver. Glyoxylate can be converted into either oxalates or glycine. Since B6 is required for the conversion into glycine, a vitamin B6 deficiency can result in the overproduction of oxalates.
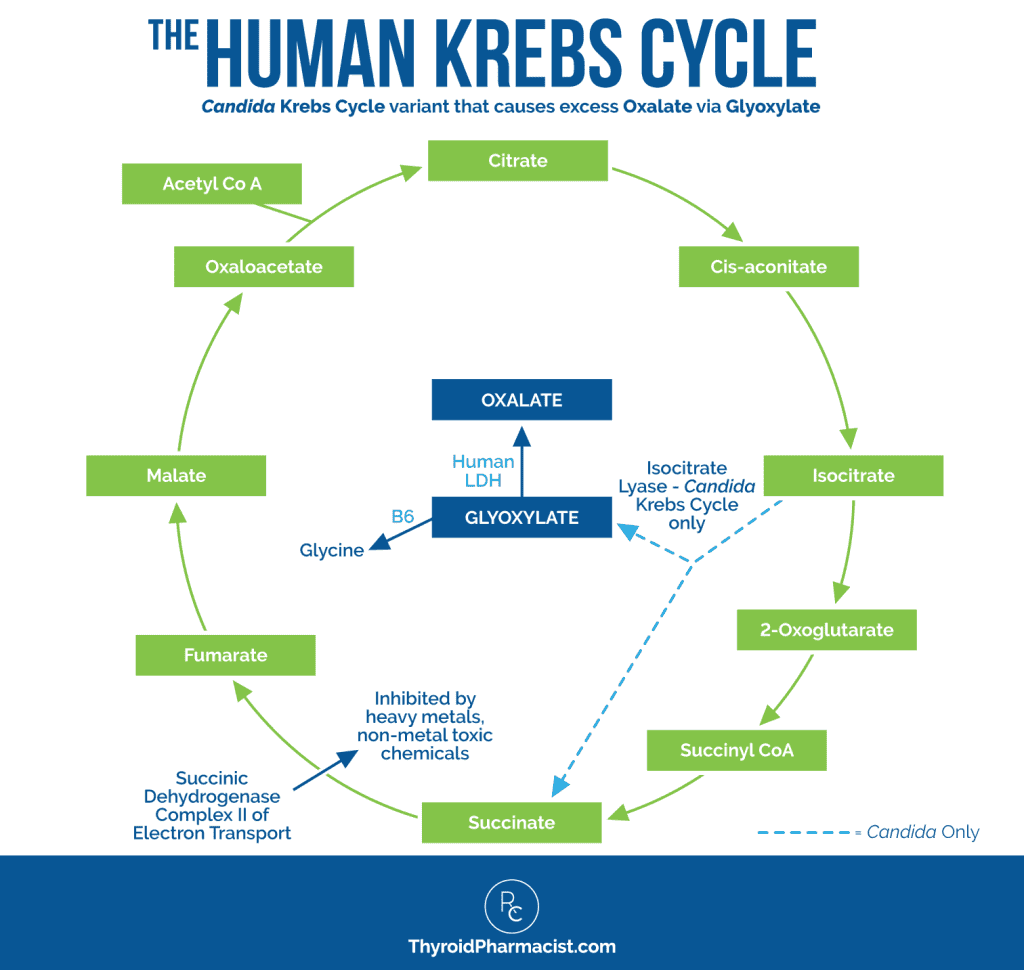
Source of original graphic: Mosaic Diagnostics. (n.d.). OAT Sample Report.
Histamines
Someone with histamine overload or intolerance may experience a number of widespread and non-specific symptoms, which can make histamine intolerance difficult to diagnose. Some of the more common symptoms include bloating along with fullness after a meal, diarrhea, abdominal pain, and constipation. Other symptoms may include headaches, low blood pressure, heart arrhythmia, hives or flushing, a runny nose, swelling in the face, mouth or throat, asthma, and fatigue. Histamine overload can also lead to insomnia, irritability, and agitation, and is associated with lowered methylation activity in the body.
The immune system releases histamines when the body is exposed to an allergic compound such as mold. Histamine then turns on an inflammatory response in order to protect the body from the offending compound.
The body can also overproduce histamines when we are colonized with fungus, H. pylori, Blasto, and other pathogenic microbes, and we can also experience symptoms when eating high histamine foods. Foods with high levels of histamines include chocolate, cheese, alcohol, cashews, avocado, and fermented foods.
The DAO (diamine oxidase) enzyme is responsible for breaking down histamines, but as you may have guessed, it’s a B6 dependent enzyme, meaning it doesn’t work adequately when we are B6 deficient.
Balancing Blood Sugar
B6 is a cofactor for enzymes that break down carbohydrates, so adequate levels help maintain healthy blood glucose levels by breaking down carbohydrates stored in the body, and converting them from glycogen to glucose (the form that can be used by our bodies for energy). B6 also supports other enzymes that break glucose down into amino acids (this process is called gluconeogenesis).
B6 Deficiencies and Hashimoto’s
When I started doing the Organic Acids Test (OAT) with people who have Hashimoto’s, I was surprised that this deficiency was so common, but it makes sense, especially considering the many symptoms that overlap!
First and foremost, we know that most people with Hashimoto’s have an impaired stress response (sometimes called adrenal dysfunction). During an acute and chronic stress phase, we burn through our B vitamins (especially B6), and this can lead to deficiency.
Additionally, since most people with Hashimoto’s have issues with digestive function that may lead to vitamin malabsorption and dysbiosis, this may impact microbial vitamin production. For example, the bacterial species Bacteroides and Prevotella produce vitamin B6 in the gut and are often missing or out of balance in Hashimoto’s. [27]
This makes perfect sense given that along with leaky gut, many common triggers for Hashimoto’s (Candida, stress, mold overgrowth, liver congestion, poor methylation/detox, malabsorption issues, poor immune health, SIBO, and gut infections) are also associated with low levels of vitamin B6.
People with Hashimoto’s also often have low stomach acid (hydrochloric acid or HCI) and a lack of digestive enzymes which are needed to break down protein and food. All of this explains why B6 deficiency isn’t usually seen alone, but will usually be found with other nutrient deficiencies (B12 is a common one) as well. [28]
Interestingly, animal studies have shown that vitamin B6 deficiency leads to hypothyroidism. Researchers found that B6 deficiency decreased thyrotropin-releasing hormone (TRH) synthesis. TRH is the hormone that tells the pituitary gland to release TSH and produce thyroid hormones. In these studies, reversing B6 deficiency led to a normalization of thyroid hormone levels. [29]
Human studies confirm an increased incidence of vitamin B deficiency in patients with Hashimoto’s. Other autoimmune conditions, such as rheumatoid arthritis, have also been found to have increased catabolism of B6, resulting in B6 deficiencies. [30]
Besides autoimmune diseases, other conditions which put people particularly at-risk of B6 deficiency include alcoholism, obesity, pregnancy (B6 is important for fetal brain development), diabetes, inflammatory bowel disease, celiac disease, kidney disease, and protein-energy malnutrition. [31]
Symptoms of Low B6
B6 deficiency can cause a lot of symptoms (mood-related symptoms in particular), as well as depression, lack of motivation, fatigue, and poor sleep.
While I always assume some level of B vitamin deficiency in people with Hashimoto’s, there are some very specific symptoms that point to low levels of B6, including:
- Poor dream recall (red flag)
- Carpal tunnel, a common condition that causes pain, tingling, and numbness in the hands and forearms (red flag)
- Symptoms of pyroluria, such as fears or phobias, sensitivities (to light, sound, and touch), social anxiety, shyness, anxiousness, and introversion (red flag)
- Histamine, oxalate, and glutamate issues, where the body cannot effectively break down these compounds (red flag)
- Low energy
- Mood issues, including anxiety, irritability, panic, depression and/or even psychosis
- Sleep disorders
- Low B12 levels despite supplementation (B6 deficiency is often found along with other nutrient deficiencies such as low B12)
- Anemia (note that along with B6, iron is also a cofactor of serotonin synthesis and is often deficient in Hashimoto’s, leading to symptoms such as panic attacks) [32]
- Nausea (as well as morning sickness in pregnant women)
- High homocysteine levels
- Sensitivity to light and sound
- A weakened immune system
- Confusion
- Seizures
- Peripheral neuropathy (tingling, pain, and numbness in the hands and/or feet)
- Cardiac issues such as atherosclerosis, early heart attack, early stroke, or thromboembolism
Causes of B6 Deficiencies
According to the National Institutes of Health, an estimated 24 percent of those in the US who do not take a supplement that includes B6, have low P5P levels, and 11 percent of those who do take supplements still have low P5P. [33] So if you are already supplementing but still suspect symptoms, you may want to look into other root causes.
This is especially important if you have Hashimoto’s and/or other risk factors, including:
- Stress: Chronic stress depletes levels of B vitamins, including B6. [34]
- Not enough B6 in the diet: Animal protein often contains the active form (P5P), resulting in greater bioavailability than plant sources (which consist mainly of pyridoxine/B6), thus people who eat a plant-based diet are more likely to require supplementation. A gluten-free diet also appears to be associated with deficiencies in B6, possibly because of the fact that we may be eating less foods (such as grains) that have both B6 and zinc. [35]
- Malabsorption: Gut dysbiosis or digestive enzyme deficiencies often found in Hashimoto’s, can cause poor absorption.
- Liver backlog: Vitamin B6 is primarily metabolized in the liver into its active form P5P, so an overburdened liver can result in deficiencies. Vitamin B6 plays a role in breaking down foods like fats, and its deficiency has been correlated with nonalcoholic fatty liver disease. A liver backlog is one of the initial root causes I look for with my Hashimoto’s clients. [36]
- Certain medications are pyridoxine-inactivating: Oral contraceptives, testosterone, NSAIDs (non-steroidal anti-inflammatory drugs), corticosteroids, barbiturates, antiseizure drugs, cycloserine, isoniazid, carbamazepine, ethionamide, penicillamine, theophylline, valproic acid and hydralazine have all been implicated as B6-inactivating medications. [37]
- Alcohol abuse: This is due to its impact on liver health and its ability to metabolize B6. [38]
- Pyroluria: Pyroluria is an abnormality in the synthesis of hemoglobin, the protein that binds iron in red blood cells. The result is that there is an overabundance of pyrroles in the body. Pyrroles bind to B6 (and other nutrients – especially zinc) which are then excreted in the urine, leading to a B6 deficiency. This chemical imbalance can cause social anxiety, shyness, and introversion, and is associated with deficiencies in B6 and zinc. [39]
- Genetics: Some people have genetic issues which may prevent them from activating pyridoxine into P5P properly. This may lead to higher B6 requirements, and/or may cause them to burn through B6 at a quicker rate. [40]
- Pregnancy: Low B6 levels are common in pregnancy, especially in women who experience nausea/vomiting and hypertension (preeclampsia). [41]
- Protein Energy Undernutrition (PEU): PEU is a disorder where a person lacks energy because they are lacking macronutrients (fat, proteins, and carbohydrates). The most extreme form would be from direct starvation (for example, from famine or anorexia), but it may also happen due to certain illnesses or disorders that decrease appetite or impair digestion. [42]
Pyroluria: Co-Occurring B6 & Zinc Deficiency
In some cases, people may have a B6 deficiency along with a zinc deficiency. This can point to pyroluria (more on that below).
Zinc is also required to convert B6 into its active form P5P. A key enzyme in the formation of vitamin B6 coenzymes, called pyridoxal kinase, requires a zinc-ATP complex (zinc-metallothionein) as a substrate to convert B6 to its active form. [43] See my article on zinc to learn more about zinc deficiency and how to boost levels.
Pyroluria (also known as pyrrole disorder) is a condition that has to do with how hemoglobin (the protein that binds iron in red blood cells) is made. The HPL (pyrrole) molecule is a byproduct of red blood cell production, which binds to B6 and zinc and is excreted through the urine. An excess of pyrroles can result in B6 and zinc loss, leading to deficiencies. [44]
In pyroluria, with the deficiency in these nutrients, there can be a profound effect on behavior, stress control, irritability threshold, and mood. People may experience emotional lability (mood swings), fears or phobias, sensitivities (to light, sound, and touch), and be easily overwhelmed. Additionally, symptoms can include those associated with “social anxiety” such as shyness, anxiousness, and introversion.
Zinc, B6, and evening primrose oil supplements in the correct dosages can help with symptoms associated with pyroluria. [45] I will be writing an article all about pyroluria in the future, so be sure to sign up for my mailing list (and get a few free gifts) for more information.
How to Know If You Are Deficient in B6
When I work with clients, I generally look at symptoms to determine if they’re deficient in B6. Poor dream recall and/or carpal tunnel are red flag giveaways that the person is deficient, so I generally recommend supplementing when a red flag symptom is present, and/or if they have more than a few B6 deficiency symptoms.
Additionally, anyone who has mental health issues or symptoms of pyroluria, histamine, oxalate and/or glutamate issues, is going to be a person that will more than likely benefit from B6 supplements! In addition to looking at your symptoms (or perhaps if you are already supplementing and wanting to see if you have adequate amounts), you may wish to do testing.
B6 Testing
Blood testing for B6 is available, but I generally prefer to use functional medicine urine tests. Blood tests don’t always provide useful info on B6 levels, as inflammation and disease states can influence results. [46] I instead prefer to use the Organic Acids Test (OAT) from Mosaic Diagnostics.
Organic acids are urinary compounds that can be useful for determining B vitamin status as well as neurotransmitter function (including deficiencies of serotonin and imbalances in dopamine and norepinephrine in particular). The test also identifies opportunistic and pathogenic digestive bacteria, yeast overgrowth, and infections.
We can get a lot of useful info relating to a wide variety of underlying issues – and their impact on mood – via this test.
Should you have your lab results from a recent routine blood test, you can take a look at the marker alanine transaminase (ALT). ALT is an enzyme found mostly in the liver, and high levels can indicate something going on in the liver. Low levels (single digits), on the other hand, can indicate a vitamin B6 deficiency or chronic kidney disease.
Advanced testing is available for vitamin and mineral deficiencies, which can be used to check levels of B6, zinc, and other nutrients often found to be deficient in Hashimoto’s. The SpectraCell Laboratories Micronutrient Test will check for multiple nutrients, including: vitamin A, vitamin B1, vitamin B2, vitamin B3, vitamin B6, vitamin B12, biotin, folate, vitamin C, vitamin D, vitamin K, calcium, magnesium, manganese, copper, selenium, vitamin E, zinc, and more!
Amino acid testing can also point to B6 deficiencies, where elevated blood amino acids would suggest an issue. Testing for amino acid deficiencies can be valuable in addressing other issues as well, such as blood sugar imbalances, food sensitivities, digestive issues, etc. This could be a viable option should you want to dig a bit more deeply into those issues.
Conventional Approach to Addressing B6 Deficiency
In conventional medicine, specific vitamin deficiencies (or nutritional root causes) are often not investigated as they would be in functional or orthomolecular medicine. Conditions such as pyroluria remain controversial in conventional medicine, and therefore may not be considered; thus, you will want to find a good functional practitioner to help you.
Because B6 deficiency impacts mood and behavior, a doctor may be more likely to assume a patient needs an antidepressant than look for a nutritional cause, and may even diagnose an individual with bipolar disorder. (I have been told more than once that I need a prescription to deal with mood, sleep, or anxiety symptoms, rather than uncover other root causes.)
Some other doctors may suspect that the cause is nutritional, yet simply suggest that a person gets more sleep, loses weight, or takes a multivitamin.
In cases where B6 is evaluated via a blood test, practitioners may consider levels of P5P at 5 to 50 µg/L a “normal” reference range. However, plasma P5P below 30 nmol/L has been used as an indicator of insufficient vitamin B6 status, while below 20 nmol/L is thought to indicate deficiency. [47]
The current recommended dietary allowance (RDA) for vitamin B6 is mainly based on plasma P5P of at least 20 nmol/L. The RDA for adults 50 and younger is 1.3 mg. After age 50, the RDA is 1.5 mg for women and 1.7 mg for men. [48]
The standard RDA for B6 is significantly lower than the therapeutic dose recommended by functional medical practitioners (generally starting at 50 mg of P5P per day).
B6 Toxicity Precautions
In pharmacy school, I learned that water-soluble vitamins were generally safe to take because they didn’t build up in the body, but that fat-soluble vitamins could pose a problem if taken in excessive amounts due to accumulation in our fat, leading to toxicity.
It’s important to know that while the B vitamins are water-soluble vitamins, the pyridoxine form of B6 is the only B vitamin that can indeed cause toxicity as well. Excessive amounts of B6 in the pyridoxine form (over 200 to 300 mg/day on an ongoing basis) may result in toxicity.
B6 toxicity typically manifests as symptoms of peripheral neuropathy, such as numbness, tingling, tremors, and twitching at body extremities. [49] Other symptoms include gastrointestinal issues, skin issues, photosensitivity, sleep disorders, hyperesthesia (sensitivity of one of the senses – e.g. sensitivity to bright lights), nausea, dizziness, and ataxia (lack of coordination and muscle control). [50]
Paradoxically, the most common symptoms associated with vitamin B6 toxicity are similar to those with vitamin B6 deficiency.
Please note that toxicity has only been associated with excessive supplementation, and not dietary overload.
Research has found that toxicity symptoms usually do not develop at doses of B6 less than 1000 mg per day; however, there are some case reports indicating sensory neuropathies at doses less than 500 mg in some patients taking B6 for months. There are no studies showing sensory nerve symptoms at a daily intake below 200 mg of B6 per day, but during my training as a pharmacist, I did learn that doses above 300 mg per day should be avoided to prevent peripheral neuropathy. [51]
The scary part of this nerve damage is that while it’s often temporary and stops when supplements are stopped, in some cases, it has been reported to be permanent. I dug into the rabbit hole of opinions and research on this, and came across some potential reasons why that may be the case.
Toxic Metabolite Theory
While pyridoxine is water soluble like the rest of the B vitamins, and generally has a short half-life (meaning it leaves the body quickly), there are opinions that there may be potential intermediate metabolites of pyridoxine that may NOT be water soluble, and/or may have long half-lives, leading to accumulation in the body.
While the research doesn’t have a clear consensus of the particular metabolite, pyridoxic acid and pyridoxine 5′-phosphate (PNP) have both been suggested to be potentially toxic metabolites.
Thus this theory suggests that the symptoms seem to stem not from actual pyridoxine accumulation, but rather from the accumulation of the intermediate metabolite(s). There may be a reason why someone can over-accumulate the intermediate metabolite, such as co-occuring zinc deficiency or a genetic variation. I haven’t been able to fact check this beyond opinions at this time, but that doesn’t mean this theory isn’t valid.
Receptor Destruction Theory
Another theory focuses on how synthetic pyridoxine, when dosed too high, may destroy P5P-dependent enzymes, preventing the proper use of the active form of B6. Because it destroys these enzymes, there is an excess of pyridoxine and not enough of the active form of vitamin B6 (P5P). [52] This theory would explain why the symptoms of B6 toxicity mimic symptoms of deficiency.
Additionally, the following reasons have been suggested as potential reasons why one may experience B6 toxicity:
- Genetics. The MTHFR is one example of a gene issue that can affect the way the body processes B6.
- Gut health status, as this affects absorption and detox capabilities.
- Other underlying health conditions such as diabetes and hormone imbalances.
- Medications that can interfere with clearance of B6 (both prescribed and over-the-counter).
- Toxins, including heavy metals, organophosphates, and ethanol (these can cause a variety of issues as well as mimic B6 toxicity).
- Nutrient deficiencies and/or excesses such as magnesium, iron, B2, B3, and zinc.
- Exposure to light like artificial light (blue light) can reduce melatonin production, for instance, whereas sunlight can stimulate serotonin.
It’s also been suggested that in some cases of peripheral neuropathy that’s thought to be caused by B6 toxicity, the reason may be something else such as autoimmune disorders, liver disease, diabetes, hypothyroidism, Lyme disease, syphilis, lymphoma, porphyria (a group of disorders that affect the skin and nervous system), and monoclonal gammopathies (conditions where antibodies are found in the blood). [53]
I know I’ve had a few clients tell me they’ve had what appear to be B6 toxicity symptoms at doses far below the toxicity warnings. One mentioned that many of her other supplements and protein powder contained B6, so it was difficult to know how much she was really taking in.
While my dear friend and nutritionist extraordinaire Trudy Scott has routinely recommended doses of B6 up to 500 mg per day for her clients and not had any negative effects, she generally uses B6 in combination with other supplements such as zinc, that may help to convert it to its active form. I have personally used up to 200 mg/daily of B6/P5P for myself, with no ill effect, as well.
For most people, staying under this level will not cause problems and if any adverse symptoms were to develop, the research indicates (and Trudy’s and my clinical experience supports) that such symptoms would reside once supplementation levels were reduced. That said, I tend to err on the side of caution, and this is why I recommend the pyridoxal 5′-phosphate (P5P) version of B6 (versus pyridoxine), as it is better absorbed and has a much lower incidence of side effects and toxicity. I discuss my recommendations below.
Root Cause Approach to Addressing Vitamin B6 Deficiency
As a root cause detective, I always look at a person’s symptoms, especially the mood and behavior-related ones that raise a red flag relating to vitamin B6 deficiency. I will also carefully review their health history timeline, taking a look for medications known to affect B6 absorption, gut and liver health, SIBO, stress, alcohol use, heavy metal exposure, and toxin exposure. I consider testing based on what I see going on, or I may just look at the standard lab markers mentioned and use the screening tools for clues.
Please note that while we can get vitamin B6 from our diet, I’ve found that increasing B6-rich foods usually doesn’t move the needle for someone with a deficiency, and supplementation can be hugely helpful.
As mentioned above, excessive amounts of vitamin B6 in the pyridoxine form can result in toxicity, which is why I almost always suggest someone uses the P5P form of B6, and starts with a low dose.
Pyridoxal-5-Phosphate (P5P): I generally suggest starting with one 50 mg capsule of P5P.
It can be taken anytime of day, with food. This supplement is a great option for those who have problems with methylation (converting B6 to P5P). The dose may be increased to 2 or 3 capsules per day.
High quality options of P5P include Rootcology P5P and the one from Pure Encapsulations.
Note: The milligrams of B6 do not equate to the milligrams of P5P – so 200 mg of B6 would be similar to 50 mg of P5P.
While most people don’t have issues with the P5P version of B6, if you notice any of the symptoms of toxicity mentioned above, reduce your dose immediately. As always, I recommend consulting with your healthcare practitioner before starting any new supplement.
Other Conditions that B6 can Help With
We’ve seen that B6 deficiency is associated with impacts to thyroid health, other altered metabolic states (pregnancy, diabetes, etc.), and pyroluria. We’ve also touched on how deficiencies in B6 levels are affected by malabsorptive states such as inflammatory bowel disease, celiac disease, and of course, Hashimoto’s. Low plasma levels of active B6 also tend to be found in alcoholics. [54] B6 supplementation can benefit these deficiencies.
B6 supplementation may also help with:
- Insomnia: B6 plays a role as a cofactor for serotonin and melatonin (our sleep hormone). [55]
- Histamine intolerance: As discussed earlier, B6 breaks down histamine in the body.
- Food sensitivities such as gluten: People on gluten-free diets may have vitamin B6 deficiencies, which can be improved by supplementation. [56]
- Carpal tunnel syndrome: Early studies have suggested that supplementation with 100-200 mg/day of B6 for several months may improve carpal tunnel syndrome (CTS) symptoms for people with low levels of B6. [57] Another study found decreased serum levels of P5P were associated with increased symptoms of CTS, including tingling, pain and nocturnal awakening. [58]
- Nausea in pregnancy: A number of studies have found B6 can help relieve pregnancy-related nausea. [59]
- PMS: Studies suggest that taking up to 100 mg/day of B6 will likely help with premenstrual syndrome symptoms and premenstrual depression. [60]
- Seizures: Supplementing with B6 may help with seizures due to rare genetic conditions relating to vitamin B6 metabolism. [61]
Final Thoughts on Vitamin B6 Deficiency
People with Hashimoto’s may be more prone to developing nutrient deficiencies, including those related to vitamin B6 levels. In my experience, supplementation can really help improve well-being and mood, especially if you are deficient.
If you do try supplementation, use caution, watch your daily dosage, and assess whether supplementation makes you feel better or worse.
If you have experienced anything to do with a B6 deficiency, please let me know below — I’d love to hear from you!
To learn more about the root causes of Hashimoto’s and how you can approach thyroid healing both naturally and sustainably, I’ve compiled years of research, personal experience and clinical outcomes into my books, Hashimoto’s: The Root Cause, Hashimoto’s Protocol, and Hashimoto’s Food Pharmacology: Nutrition Protocols and Healing Recipes to Take Charge of Your Thyroid Health. My newest book, Adrenal Transformation Protocol, details a gentle protocol for uncovering and healing adrenal dysfunction — this can help you address emotional and psychological stress as well.
As always, I wish you the best on your journey toward better health!
P.S. I love staying in touch with my readers! To stay on top of thyroid health updates and meet others who are following similar health journeys, please join my Facebook, Instagram, TikTok, and Pinterest community pages. For recipes, a Thyroid Diet start guide, notifications about upcoming events, and the Nutrient Depletions and Digestion chapter from my first book for free, be sure to sign up for my email list!
References
[1] Mooney S, Leuendorf JE, Hendrickson C, Hellmann H. Vitamin B6: a long known compound of surprising complexity. Molecules. 2009;14(1):329-351. Published 2009 Jan 12. doi:10.3390/molecules14010329; Vitamin B6 Fact Sheet for Health Professionals. National Institutes of Health Office of Dietary Supplements. Updated June 2, 2022. Accessed May 15, 2023. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional/; Parra M, Stahl S, Hellmann H. Vitamin B₆ and Its Role in Cell Metabolism and Physiology. Cells. 2018;7(7):84. Published 2018 Jul 22. doi:10.3390/cells7070084
[2] Ods.od.nih.gov. 2021. Office of Dietary Supplements. Vitamin B6. National Institute Of Health. Updated 2021. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional/. Accessed 11 February 2022.
[3] Parra M, Stahl S, Hellmann H. Vitamin B₆ and Its Role in Cell Metabolism and Physiology. Cells. 2018;7(7):84. Published 2018 Jul 22. doi:10.3390/cells7070084
[4] Dhalla NS, Takeda S, Elimban V. Mechanisms of the beneficial effects of vitamin B6 and pyridoxal 5-phosphate on cardiac performance in ischemic heart disease. Clin Chem Lab Med. 2013;51(3):535-543. doi:10.1515/cclm-2012-0553
[5] Stover PJ, Field MS. Vitamin B-6. Adv Nutr. 2015;6(1):132-133. Published 2015 Jan 15. doi:10.3945/an.113.005207
[6] Peuhkuri K, Sihvola N, Korpela R. Dietary factors and fluctuating levels of melatonin. Food Nutr Res. 2012;56:10.3402/fnr.v56i0.17252. doi:10.3402/fnr.v56i0.17252
[7] Field DT, Cracknell RO, Eastwood JR, et al. High-dose Vitamin B6 supplementation reduces anxiety and strengthens visual surround suppression. Hum Psychopharmacol. 2022;37(6):e2852. doi:10.1002/hup.2852; McCarty MF. High-dose pyridoxine as an ‘anti-stress’ strategy. Med Hypotheses. 2000;54(5):803-807. doi:10.1054/mehy.1999.0955
[8] Appleton J. The Gut-Brain Axis: Influence of Microbiota on Mood and Mental Health. Integr Med (Encinitas). 2018;17(4):28-32.
[9] Banskota S, Ghia JE, Khan WI. Serotonin in the gut: Blessing or a curse. Biochimie. 2019 Jun;161:56-64. doi: 10.1016/j.biochi.2018.06.008.
[10] Dukowicz AC, Lacy BE, Levine GM. Small intestinal bacterial overgrowth: a comprehensive review. Gastroenterol Hepatol (N Y). 2007;3(2):112-122; Patil AD. Link between hypothyroidism and small intestinal bacterial overgrowth. Indian J Endocrinol Metab. 2014;18(3):307-309. doi:10.4103/2230-8210.131155
[11] Ligaarden SC, Farup PG. Low intake of vitamin B6 is associated with irritable bowel syndrome symptoms. Nutr Res. 2011 May;31(5):356-61. doi: 10.1016/j.nutres.2011.04.001; Sikander A, Rana SV, Prasad KK. Role of serotonin in gastrointestinal motility and irritable bowel syndrome. Clin Chim Acta. 2009 May;403(1-2):47-55. doi: 10.1016/j.cca.2009.01.028; Fayyaz M, Lackner JM. Serotonin receptor modulators in the treatment of irritable bowel syndrome. Ther Clin Risk Manag. 2008;4(1):41-48. doi:10.2147/tcrm.s140
[12] Yoshii K, Hosomi K, Sawane K, et al. Metabolism of dietary and microbial vitamin B family in the regulation of host immunity. Front Nutr. 2019;6:48. Published 2019 Apr 17. doi:10.3389/fnut.2019.00048
[13] Paul L, Ueland PM, Selhub J. Mechanistic perspective on the relationship between pyridoxal 5′-phosphate and inflammation. Nutr Rev. 2013;71(4):239-244. doi:10.1111/nure.12014; Sakakeeny L, Roubenoff R, Obin M, et al. Plasma pyridoxal-5-phosphate is inversely associated with systemic markers of inflammation in a population of U.S. adults. J Nutr. 2012;142(7):1280-1285. doi:10.3945/jn.111.153056
[14] Zhang XH, Ma J, Smith-Warner SA, et al. Vitamin B6 and colorectal cancer: current evidence and future directions. World J Gastroenterol. 2013;19(7):1005-1010. doi:10.3748/wjg.v19.i7.1005;Stach K, Stach W, Augoff K. Vitamin B6 in health and disease. Nutrients. 2021;13(9):3229. Published 2021 Sep 17. doi:10.3390/nu13093229; Qian B, Shen S, Zhang J, et al. Effects of vitamin B6 deficiency on the composition and functional potential of T cell populations. J Immunol Res. 2017;2017:2197975. doi: 10.1155/2017/2197975; Yoshii K, Hosomi K, Sawane K, et al. Metabolism of dietary and microbial vitamin B family in the regulation of host immunity. Front Nutr. 2019;6:48. Published 2019 Apr 17. doi:10.3389/fnut.2019.00048; Herr N, Bode C, Duerschmied D. The effects of serotonin in immune cells. Front Cardiovasc Med. 2017;4:48. Published 2017 Jul 20. doi:10.3389/fcvm.2017.00048; Brown MJ, Ameer MA, Beier K. Vitamin B6 deficiency. [Updated 2021 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579/
[15] Durga J, van Tits LJ, Schouten EG, Kok FJ, Verhoef P. Effect of lowering of homocysteine levels on inflammatory markers: a randomized controlled trial. Arch Intern Med. 2005;165(12):1388-1394. doi:10.1001/archinte.165.12.1388; Vitamin B6 Fact Sheet for Health Professionals. National Institutes of Health Office of Dietary Supplements. Updated June 2, 2022. Accessed May 15, 2023. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional/
[16] Thakur P, Bhalerao A. High Homocysteine Levels During Pregnancy and Its Association With Placenta-Mediated Complications: A Scoping Review. Cureus. 2023;15(2):e35244. Published 2023 Feb 20. doi:10.7759/cureus.35244
[17] Ganguly P, Alam SF. Role of homocysteine in the development of cardiovascular disease. Nutr J. 2015;14:6. Published 2015 Jan 10. doi:10.1186/1475-2891-14-6
[18] Chiocchetti A, Prodam F, Dianzani U. Homocysteine and Folate in Inflammatory Bowel Disease: Can Reducing Sulfur Reduce Suffering?. Dig Dis Sci. 2018;63(12):3161-3163. doi:10.1007/s10620-018-5274-2
[19] Camfield DA, Wetherell MA, Scholey AB, et al. The effects of multivitamin supplementation on diurnal cortisol secretion and perceived stress. Nutrients. 2013;5(11):4429-4450. Published 2013 Nov 11. doi:10.3390/nu5114429
[20] Shulpekova YO, Nechaev VM, Popova IR, et al. Food Intolerance: The Role of Histamine. Nutrients. 2021;13(9):3207. Published 2021 Sep 15. doi:10.3390/nu13093207
[21] Ferraro PM, Taylor EN, Gambaro G, Curhan GC. Vitamin B6 intake and the risk of incident kidney stones. Urolithiasis. 2018;46(3):265-270. doi:10.1007/s00240-017-0999-5
[22] Folkers K, Shizukuishi S, Willis R, Scudder SL, Takemura K, Longenecker JB. The biochemistry of vitamin B6 is basic to the cause of the Chinese restaurant syndrome. Hoppe Seylers Z Physiol Chem. 1984;365(3):405-414. doi:10.1515/bchm2.1984.365.1.405
[23] Folkers K, Shizukuishi S, Willis R, Scudder SL, et al.The biochemistry of vitamin B6 is basic to the cause of the Chinese restaurant syndrome. Hoppe Seylers Z Physiol Chem. 1984 Mar;365(3):405-14. doi: 10.1515/bchm2.1984.365.1.405.
[24] Holton KF, Kirkland AE, Baron M, et al. The low glutamate diet effectively improves pain and other symptoms of gulf war illness. Nutrients. 2020;12(9):2593. Published 2020 Aug 26. doi:10.3390/nu12092593
[25] Reid JD, Choi CH, Oldroyd NO. Calcium oxalate crystals in the thyroid. Their identification, prevalence, origin, and possible significance. Am J Clin Pathol. 1987;87(4):443-454. doi:10.1093/ajcp/87.4.443
[26] Curhan GC, Willett WC, Speizer FE, Stampfer MJ. Intake of vitamins B6 and C and the risk of kidney stones in women. J Am Soc Nephrol. 1999;10(4):840-845. doi:10.1681/ASN.V104840
[27] Brown MJ, Ameer MA, Beier K. Vitamin B6 deficiency. [Updated 2021 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579/; Mayengbam S, Chleilat F, Reimer RA. Dietary vitamin B6 deficiency impairs gut microbiota and host and microbial metabolites in rats. Biomedicines. 2020;8(11):469. Published 2020 Nov 2. doi:10.3390/biomedicines8110469; Brown MJ, Ameer MA, Beier K. Vitamin B6 deficiency. [Updated 2021 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579/; Zhao F, Feng J, Li J, et al. Alterations of the gut microbiota in Hashimoto’s Thyroiditis patients. Thyroid. 2018 Feb;28(2):175-186. doi: 10.1089/thy.2017.0395
[28] Long SJ, Benton D. Effects of vitamin and mineral supplementation on stress, mild psychiatric symptoms, and mood in nonclinical samples: a meta-analysis. Psychosom Med. 2013 Feb;75(2):144-53. doi: 10.1097/PSY.0b013e31827d5fbd; Brown MJ, Ameer MA, Beier K. Vitamin B6 deficiency. [Updated 2021 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579/; Kobayashi T, Kessoku T, Ozaki A, et al. Vitamin B6 efficacy in the treatment of nonalcoholic fatty liver disease: an open-label, single-arm, single-center trial. J Clin Biochem Nutr. 2021;68(2):181-186. doi:10.3164/jcbn.20-142
[29] Sworczak K, Wiśniewski P. The role of vitamins in the prevention and treatment of thyroid disorders. Endokrynol Pol. 2011;62(4):340-4. PMID: 21879475.
[30] Kawicka A, Regulska-Ilow B, Regulska-Ilow B. Metabolic disorders and nutritional status in autoimmune thyroid diseases. Postepy Hig Med Dosw (Online). 2015 Jan 2;69:80-90. doi: 10.5604/17322693.1136383; Rose DP. The interactions between vitamin B6 and hormones. Vitam Horm. 1978;36:53-99. doi: 10.1016/s0083-6729(08)60982-6. PMID: 217175; Brown MJ, Ameer MA, Beier K. Vitamin B6 deficiency. [Updated 2021 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579/
[31] Mascolo E, Vernì F. Vitamin B6 and diabetes: relationship and molecular mechanisms. Int J Mol Sci. 2020;21(10):3669. Published 2020 May 23. doi:10.3390/ijms21103669; Brown MJ, Ameer MA, Beier K. Vitamin B6 deficiency. [Updated 2021 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579/
[32] Mikawa Y, Mizobuchi S, Egi M, et al. Low serum concentrations of vitamin B6 and iron are related to panic attack and hyperventilation attack. Acta Med Okayama. 2013;67(2):99-104. doi: 10.18926/AMO/49668.
[33] Vitamin B6 Fact Sheet for Health Professionals. National Institutes of Health Office of Dietary Supplements. Updated June 2, 2022. Accessed July 25, 2023. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional/
[34] Stough C, Simpson T, Lomas J, et al. Reducing occupational stress with a B-vitamin focussed intervention: a randomized clinical trial: study protocol. Nutr J. 2014;13(1):122. Published 2014 Dec 22. doi:10.1186/1475-2891-13-122
[35] Brown MJ, Ameer MA, Beier K. Vitamin B6 deficiency. [Updated 2021 Dec 29]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK470579/; Stach K, Stach W, Augoff K. Vitamin B6 in Health and Disease. Nutrients. 2021;13(9):3229. Published 2021 Sep 17. doi:10.3390/nu13093229; Vitamin B6. Office of Dietary Supplements. National Institutes of Health. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional/ Updated March 26, 2021. Accessed February 18, 2022; Lerner A, O’Bryan T, Matthias T. Navigating the gluten free boom: The dark side of gluten free diet. Front Pediatr. 2019 Oct 15;7:414. doi: 10.3389/fped.2019.00414; Rondanelli M, Faliva MA, Gasparri C, et al. Micronutrients dietary supplementation advices for celiac patients on long-term gluten-free diet with good compliance: A review. Medicina (Kaunas). 2019;55(7):337. Published 2019 Jul 3. doi:10.3390/medicina55070337
[36] Labadarios D, Rossouw JE, McConnell JB, et al. Vitamin B6 deficiency in chronic liver disease–evidence for increased degradation of pyridoxal-5′-phosphate. Gut. 1977;18(1):23-27. doi:10.1136/gut.18.1.23; Kobayashi T, Kessoku T, Ozaki A, et al. Vitamin B6 efficacy in the treatment of nonalcoholic fatty liver disease: an open-label, single-arm, single-center trial. J Clin Biochem Nutr. 2021;68(2):181-186. doi:10.3164/jcbn.20-142
[37] Larry E. Johnson. Vitamin B6 Deficiency and Dependency. Merckmanuals.com. https://www.merckmanuals.com/professional/nutritional-disorders/vitamin-deficiency,-dependency,-and-toxicity/vitamin-b6-deficiency-and-dependency. Updated November 2020. Accessed February 18, 2022.
[38] Vech RL, Lumeng L, Li TK. Vitamin B6 metabolism in chronic alcohol abuse The effect of ethanol oxidation on hepatic pyridoxal 5′-phosphate metabolism. J Clin Invest. 1975;55(5):1026-1032. doi:10.1172/JCI108003
[39] Warren B, Sarris J, Mulder RT, Rucklidge JJ. Pyroluria: Fact or Fiction?. J Altern Complement Med. 2021;27(5):407-415. doi:10.1089/acm.2020.0151
[40] Tanaka T, Scheet P, Giusti B, et al. Genome-wide association study of vitamin B6, vitamin B12, folate, and homocysteine blood concentrations [published correction appears in Am J Hum Genet. 2009 May;84(5):712]. Am J Hum Genet. 2009;84(4):477-482. doi:10.1016/j.ajhg.2009.02.011
[41] Vitamin B6 Fact Sheet for Health Professionals. National Institutes of Health Office of Dietary Supplements. Updated June 2, 2022. Accessed May 15, 2023. https://ods.od.nih.gov/factsheets/VitaminB6-HealthProfessional/
[42] Morley, JE. Protein-Energy Undernutrition (PEU). Merck Manual. Updated September 2022. Reviewed July 2021. https://www.merckmanuals.com/en-ca/professional/nutritional-disorders/undernutrition/protein-energy-undernutrition-peu
[43] Zinc and the regulation of vitamin B6 metabolism. Nutr Rev. 1990 Jun;48(6):255-8. doi: 10.1111/j.1753-4887.1990.tb02951.x; Pillay D, Gathiram P, Ubbink JB. Zinc status in vitamin B6 deficiency. Int J Vitam Nutr Res. 1997;67(1):22-6; Mensah, Albert. Webinar: Facts & Myths about Pyrrole Disorder: Learn how Polyuria Impacts Emotional & Mental Health. Mensah Medical. Presented Thursday, June 19, 2014. Accessed May 11, 2023. https://www.youtube.com/watch?v=kyjTY0Rjl_Q
[44] Jurnak F. The pivotal role of aldehyde toxicity in autism spectrum disorder: The therapeutic potential of micronutrient supplementation. Nutr Metab Insights. 2016 Jun 14;8(Suppl 1):57-77. doi: 10.4137/NMI.S29531.
[45] Warren B, Sarris J, Mulder RT, Rucklidge JJ. Pyroluria: Fact or Fiction?. J Altern Complement Med. 2021;27(5):407-415. doi:10.1089/acm.2020.0151
[46] Ueland PM, Ulvik A, Rios-Avila L, et al. Direct and functional biomarkers of vitamin B6 status. Annu Rev Nutr. 2015;35:33-70. doi:10.1146/annurev-nutr-071714-034330
[47] Ashwin Pai. Vitamin B6. Emedicine.Medscape.com. https://emedicine.medscape.com/article/2088627-overview Updated April 01, 2014. Accessed February 17, 2022; Ye X, Maras JE, Bakun PJ, et al.Dietary intake of vitamin B-6, plasma pyridoxal 5′-phosphate, and homocysteine in Puerto Rican adults. J Am Diet Assoc. 2010;110(11):1660-1668. doi:10.1016/j.jada.2010.08.006
[48] Ye X, Maras JE, Bakun PJ, et al. Dietary intake of vitamin B-6, plasma pyridoxal 5′-phosphate, and homocysteine in Puerto Rican adults. J Am Diet Assoc. 2010;110(11):1660-1668. doi:10.1016/j.jada.2010.08.006; Vitamin B-6. Mayo Clinic. Updated Feb 3, 2021. Accessed June 16, 2023. https://www.mayoclinic.org/drugs-supplements-vitamin-b6/art-20363468
[49] Katan MB. Hoeveel vitamine B6 is toxisch? [How much vitamin B6 is toxic?]. Ned Tijdschr Geneeskd. 2005;149(46):2545-2546.
[50] Hemminger A, Wills BK. Vitamin B6 Toxicity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 7, 2023.
[51] Hemminger A, Wills BK. Vitamin B6 toxicity. [Updated 2022 Jan 10]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK554500/
[52] Vrolijk MF, Opperhuizen A, Jansen EHJM, Hageman GJ, Bast A, Haenen GRMM. The vitamin B6 paradox: Supplementation with high concentrations of pyridoxine leads to decreased vitamin B6 function. Toxicol In Vitro. 2017;44:206-212. doi:10.1016/j.tiv.2017.07.009; Hemminger A, Wills BK. Vitamin B6 Toxicity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; February 7, 2023.
[53] Ibid.
[54] Gramlich L., et al. Nutritional Status in Patients with Heavy Alcohol Use. UpToDate. May 2023. Accessed June 24, 2023. https://www-uptodate-com.mwu.idm.oclc.org/contents/nutritional-status-in-patients-with-sustained-heavy-alcohol-use
[55] Pyridoxine (vitamin B6) influence on endogenic melatonin production during the experiment. Georgian Med News. 2007 Dec;(153):35-8. Russian. PMID: 18250494; Djokic G, Vojvodić P, Korcok D, et al. The effects of magnesium – melatonin – vit B complex supplementation in treatment of insomnia. Open Access Maced J Med Sci. 2019 Aug 30;7(18):3101-3105. doi: 10.3889/oamjms.2019.771; Baldewicz T, Goodkin K, Feaster DJ, et al. Plasma pyridoxine deficiency is related to increased psychological distress in recently bereaved homosexual men. Psychosom Med. 1998 May-Jun;60(3):297-308. doi: 10.1097/00006842-199805000-00016; Kennedy DO. B vitamins and the brain: Mechanisms, dose and efficacy–A review. Nutrients. 2016;8(2):68. Published 2016 Jan 27. doi:10.3390/nu8020068
[56] Hallert C, Grant C, Grehn S, et al. Evidence of poor vitamin status in coeliac patients on a gluten-free diet for 10 years. Aliment Pharmacol Ther. 2002 Jul;16(7):1333-9. doi: 10.1046/j.1365-2036.2002.01283.x.
[57] Vitamin B6. Linus Pauling Institute. Oregon State University. https://lpi.oregonstate.edu/mic/vitamins/vitamin-B6 Published 2000. Updated 2014. Accessed February 17, 2022.
[58] Ibid; Calderón-Ospina, Carlos Alberto, and Mauricio Orlando Nava-Mesa. B vitamins in the nervous system: Current knowledge of the biochemical modes of action and synergies of thiamine, pyridoxine, and cobalamin. CNS neuroscience & therapeutics vol. 26,1 (2020): 5-13. doi:10.1111/cns.13207
[59] Ibid.
[60] Wyatt KM, Dimmock PW, Jones PW, et al. Efficacy of vitamin B-6 in the treatment of premenstrual syndrome: systematic review. BMJ. 1999 May 22;318(7195):1375-81. doi: 10.1136/bmj.318.7195.1375; Doll H, Brown S, Thurston A, et al. Pyridoxine (vitamin B6) and the premenstrual syndrome: a randomized crossover trial. J R Coll Gen Pract. 1989 Sep;39(326):364-8.
[61] Vitamin B6. Linus Pauling Institute. Oregon State University. https://lpi.oregonstate.edu/mic/vitamins/vitamin-B6 Published 2000. Updated 2014. Accessed February 17, 2022.

Dear Isabella, This is such a helpful article to me! I have histamine intolerance, menstrual related migraines, fat malabsorption, and fungal nail infections. I also have Hashimotos and two variations of the MTHFR gene. But I have also experienced weird symptoms taking B6, for instance, the tip of my tongue went numb, so I have not taken it on a regular basis. I have all the red flags. I also tested extremely high on a blood B12 test which I read could indicate a deficiency, but the doctor told me to just stop what I was doing. (But I wasn’t taking any B supplements!) I am just cautious about supplementation. I have tried B6, P5P, and multi B vitamins. This article will help me try again and watch for toxicity. It really does sound like you are onto something. Thank you so much! Please reply if you have the time. I would really appreciate it!
Jennifer – thank you for sharing your journey. I’m so sorry you are struggling with all of these symptoms. Being cautious when supplementing is a good thing. I have some articles on some of these including MTHFR if you would like to check those out to see if they can be helpful. I also highly recommend that you work with a functional medicine clinician to be a part of your own health care team. It’s an entire medical specialty dedicated to finding and treating underlying root causes and preventing serious chronic disease rather than treating individual disease symptoms. Check out this article:
FUNCTIONAL MEDICINE APPROACH TO THE THYROID
https://thyroidpharmacist.com/articles/functional-medicine-approach-to-the-thyroid
CLINICIAN DATABASE
https://thyroidpharmacist.com/database-recommended-clinicians/
FIND A FUNCTIONAL MEDICINE CLINICIAN
https://ifm.org/find-a-practitioner/
Recommended Compounding Pharmacist list
https://thyroidpharmacist.com/database-recommended-compounding-pharmacies/
I find this information so interesting and helpful. I definitely have almost all of the symptoms of a B6 deficiency and it makes sense. I just recently started to supplement with B6 so we will see how it goes. I had always thought I was very sensitive to it, but now I I realize it was probably the type of B6 I was taking that was the problem.
Lisa – thank you so much for sharing! I hope you will keep me posted on your progress. ❤️
My story is a bit different, but symptoms seem the same. I have gait issues, neuropathy, and many B6 deficiency issues. I stopped taking a B omplex about a month ago (ran out temporarily) and noticed I was a bit better. Symptoms seem to get worse when I eat foods with B6. The doctor did a blood test and B6 was 40 which is about double the max ref range at Quest. Also my TSH was 6.24 with fT4 1.1 fT3 2.6. Is there a way to lower B6? Any ideas in general?
Tracy – thank you for sharing your experience. As I stated in the article there are a few possible reasons for toxicity issues. I’m glad to hear that you saw improvement by stopping the supplement. I recommend discussing your symptoms with your practitioner who is familiar with your health conditions so that they can help you determine what will work best for you going forward. ❤️
What could someone do if B6 was high, but they are not taking any supplements. My husband has the deficiency symptoms you described here, but without taking B vitamins.
Hi Joyce thank you for following. I’m not sure what testing your husband had that showed he has high B6, but as I said in the article, I generally prefer to using functional medicine urine tests. Blood tests don’t always provide useful info on B6 levels, as inflammation and disease states can influence results. I instead prefer to use the Organic Acids Test (OAT) from Mosaic Diagnostics. You may also want to check any other supplements he may be getting B6 from such as a multivitamin and certainly discuss with your practitioner to help you determine what may be causing this. I do hope you will keep me posted on his progress. ❤️
Your book has been a great resource to help my Sister in law with hashimoto’s. Thank you.
Curious..What does it mean if B6 is above normal, but they are not taking any?
Tracy, You may want to check any other supplements that you may be getting B6 from such as a multivitamin and certainly discuss with your practitioner to help you determine what may be causing this. Also, I’m not sure what form of testing showed high B6, but as I said in the article, I generally prefer using functional medicine urine tests. Blood tests don’t always provide useful info on B6 levels, as inflammation and disease states can influence results. I instead prefer to use the Organic Acids Test (OAT) from Mosaic Diagnostics.
Hello Dr. Wentz!
Thank you so much for sharing your expertise regarding vitamin B6. For those of us who have interstitial cystitis and endometriosis, would you recommend taking 50 mg of the P5P form of B6, or would you recommend taking a B vitamin complex vitamin (that uses the P5P form of B6 in addition to B12)?
Thank you so much in advance for your time and assistance!
Kristin – I’m so glad this information was helpful! In my protocols, I often recommend the active P5P form of vitamin B6, especially for individuals with specific needs like supporting neurotransmitter balance and hormone metabolism. Whether to take P5P alone or as part of a B-complex can depend on your overall nutrient status, other B-vitamin needs, and any sensitivities you may have. It’s best to discuss your specific situation with a knowledgeable healthcare provider who can help determine the right dose and formulation for you, monitor your symptoms, and ensure it fits safely with any other supplements or medications you may be taking.
Thank you so much for this article, Dr. Wentz! There is so much great information here. I just wanted to comment on B6 toxicity, which I and my daughter have. My daughter (and the rest of my family) was diagnosed with Pyroluria and were taking 200 mg each of B6 and P5P. I was only taking 50 mg of P5P (I have Hashis, but not Pyroluria). I decided to try the same dose as my family and that’s when the toxicity hit (neuropathy). Then my daughter started having neuropathy as well. We both stopped taking both forms immediately. After several months break, I slowly reintroduced them to her and she does fine, now, on 100 mg each. I, however, found that for a long time I couldn’t even tolerate high B6 foods such as meat and potatoes. Now I can handle a moderate amount, but I supplement with Fenugreek when the neuropathy gets too painful.
I strongly suspect that in our case, mercury is the culprit in making it difficult for our bodies to process and excrete excess B6. We are now using the Andy Cutler method to chelate mercury. It’s a long process. I had 4 amalgams since childhood and 1 crown packed with amalgam in my 20s. I believe this was one of many triggers for my Hashimotos as well. After the crown was placed, my health quickly deteriorated and my thyroid was all but dead. My first TSH lab read 143!
Anyway, I just wanted to share my experience in hopes that it may help someone else with B6 toxicity. It’s still such a mystery. The longer I chelate, the more B6 foods I can eat without pain.
Thanks for all your incredible work.
Hi Sonja, Thank you so much for sharing your detailed experience! I’m glad you and your daughter have found a way to carefully reintroduce B6 and P5P while managing symptoms. B6 toxicity can be serious, and as you noted, individual factors like heavy metal exposure may affect how the body processes nutrients. Your story highlights the importance of working closely with a knowledgeable practitioner, listening to your body, and personalizing supplementation. I really appreciate you sharing this—it will be helpful to others navigating similar challenges.
Thanks for writing this article, I learned a lot.
I was taking magnesium glycinate daily for about 5 months, about 4 years ago.
At first, everything was fine. But after some time, I developed severe sleep maintenance insomnia, waking up and not being able to fall back to sleep.
When I stopped taking it, my sleep improved a lot, but never fully went back to normal, even 4 years later. I believe the magnesium glycinate possibly created some sort of glutamate sensitivity or imbalance, like you mention is this article. Not many people talk about this.
I am interested in trying the p5p, but the side effects sound scary, and I am extremely reluctant to take any supplement after what happened with the magnesium glycinate.
I would never take anything daily again, especially for an extended period of time. But I’m considering testing some small doses of p5p to see if it could rebalance my glutamate receptors or whatever was initially thrown off by the magnesium glycinate.
Jeremy, Thank you for sharing your experience. I’m so sorry you had that reaction. Everyone can respond to supplements differently, and I always encourage people to listen to their bodies and work with a knowledgeable practitioner when introducing anything new. When someone is very sensitive, I generally recommend starting low, going very slow, and introducing only one supplement at a time so it’s easier to monitor tolerance. 😊