If you’re reading this, then you’ve likely been faced with a “wastebasket” diagnosis. A wastebasket diagnosis is a vague diagnosis given to a person with obvious symptoms, but no clearly “identifiable medical condition,” such as chronic fatigue syndrome, irritable bowel syndrome, seronegative rheumatoid arthritis, fibromyalgia, interstitial cystitis, or subclinical hypothyroidism.
Patients with this type of condition are often looked down upon, and I’m not proud of this, but during pharmacy school, I often wondered if those conditions were even “real.” I know that, unfortunately, many healthcare professionals share that same thought process.
Why? Because people with these conditions often do not show “abnormal” test results on their standard lab tests.
How many of you have been in this situation? You go to the doctor because you have symptoms like fatigue, brain fog, and weight gain. You get your thyroid tested, and then you’re told that your labs normal, and you just need to eat less and exercise more and are given a prescription for an antidepressant.

Meanwhile, you get your test results, and you notice that your TSH was 7.99 μIU/mL —when 8 μIU/mL is considered elevated—and your doctor says that nothing can be done until you’re above the threshold.
In a recent article, The New York Times suggested that elderly people with subclinical hypothyroidism were actually not tired because of their thyroid conditions, rather they were tired because of “ennui” {definition: a feeling of listlessness and dissatisfaction arising from a lack of occupation or excitement}. (2)
They came to this conclusion because levothyroxine did not give the patient more energy or make them lose weight, and it didn’t make them “physically stronger or mentally faster.” (2)
I happen to be the Thyroid Pharmacist, so you may say that I know a thing or two about thyroid medications… My book on treating thyroid disease was a #1 New York Times bestseller, yet I was never asked to comment on proper use of thyroid hormones for the New York Times article, so I decided to post on my blog to make sure that people are properly educated so that they can advocate for themselves!
The NYT published this article because of a recent study in the New England Journal of Medicine (as I like to call it “The Missed the Forest for the Trees Study”). This study concluded that there was no benefit for elderly patients with subclinical hypothyroidism to receive thyroid treatment. (3)
Based on my experience as a pharmacist and patient advocate specializing in thyroid disorders, I find the suggestions and conclusions in both of these articles quite offensive, short-sighted, and simply wrong. Instead, I would advocate for appropriate and individualized medication management. Here’s why:
Ignoring the Patient’s Symptoms Will Not Make Them Go Away
“You’re tired because you’re getting older” is an insult to people who are seeking a professional’s help and is seldom true. I personally was told that my thyroid symptoms were due to advancing age—at age 25.
While fatigue is common, that does not mean that it’s optimal or even normal. It’s like telling someone that since cancer is common, it’s normal for them to have cancer.
The Patients Were Not Dosed Properly on the Hormones
In the study, the average TSH of the “treated” patients was 3.63±2.11 μIU/mL. In my clinical experience, most people feel their best with a TSH between 0.5-2 μIU/mL. Many patients are symptomatic with a TSH above 2.5 μIU/mL. I personally felt like a sloth with a TSH of 4 μIU/mL. How could anyone conclude that the medications were of no benefit when the medications were never dosed appropriately? It’s like saying that birth control pills don’t work when you’re only taking ½ of the effective dose to prevent pregnancy.
The Care Wasn’t Individualized
I would also like to add that the study only utilized levothyroxine. From my experience as a pharmacist, many thyroid patients actually feel significantly better with the addition of another thyroid hormone, T3 into their regimen.
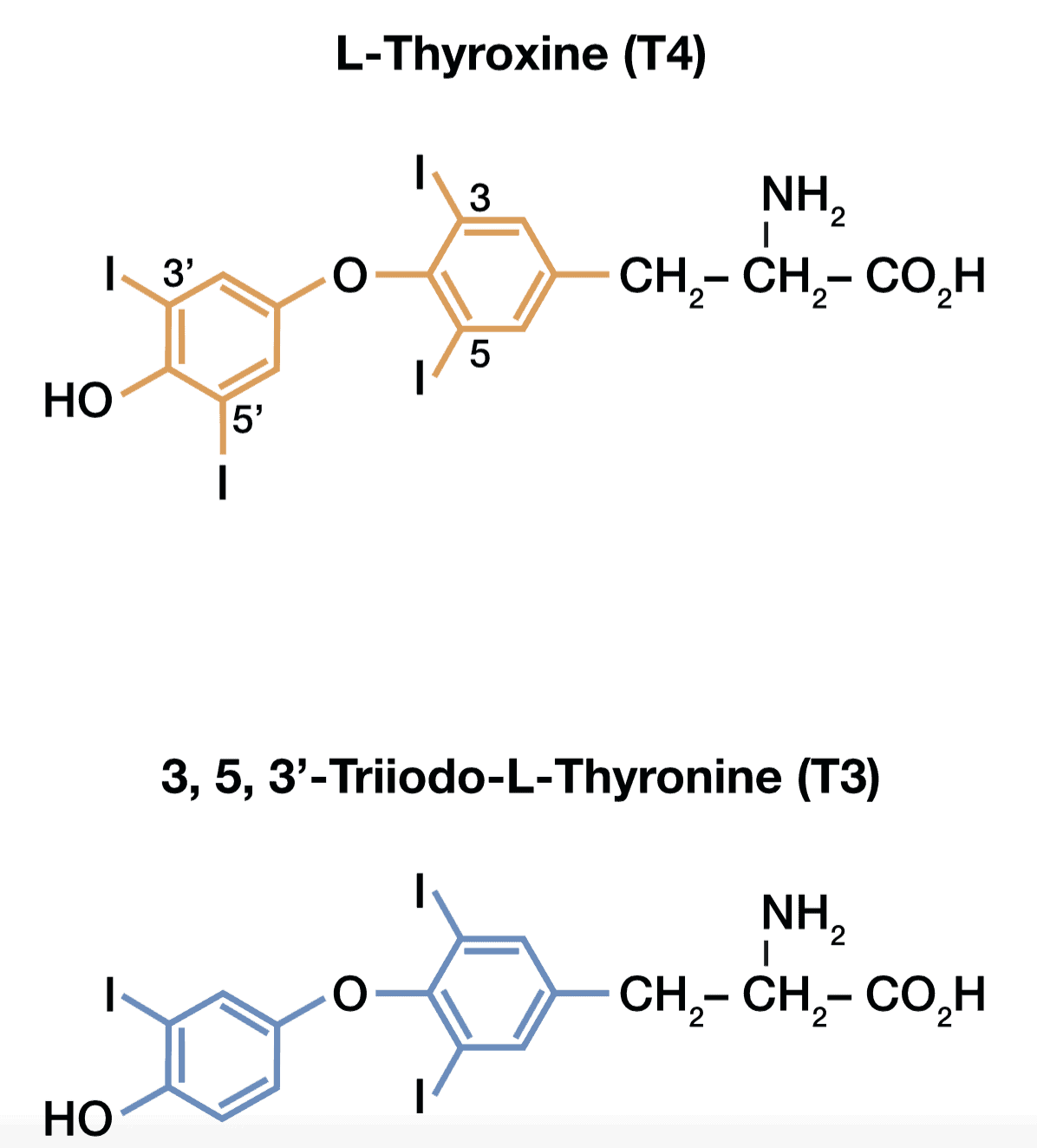
There are four main thyroid hormones that have been identified. T1, T2, T3, and T4.
T4 (Thyroxine) and T3 (Triiodothyronine) are the two main biologically active thyroid hormones. T4 is known as prohormone, which means that it needs to be converted by the body into a more active version. T4 is 300% less biologically active than T3, the main biologically active thyroid hormone.
On paper, T4 gets converted to T3 just fine; in the human body, this can be a different story. There are many factors that may inhibit proper T4 to T3 conversion, such as zinc deficiency, which is a common nutrient depletion in the elderly.
In 2014, Dr. Wilmar Wiersinga, a Dutch endocrinologist and top thyroid researcher, concluded that: “Evidence is mounting that levothyroxine monotherapy cannot assure a euthyroid state in all tissues simultaneously and that normal serum TSH levels in patients receiving levothyroxine reflect pituitary euthyroidism alone.” (4)
Dr. Wiersinga suggests that people with specific genetic polymorphisms in thyroid hormone transport may benefit from combination T4/T3 therapy and that people who continue to have thyroid symptoms despite normal TSH levels may benefit from a trial of T3 medication. (4)
Studies like this are an important reminder that we need to individualize and optimize medication therapy.
I would also like to add that all patients deserve comprehensive care and that the elderly should not be dismissed when they struggle with symptoms.
Starting Hormones in Subclinical Hypothyroidism Can Help with Slowing Down Disease Progression
Ninety-five percent of thyroid disease in Western countries develops due to an autoimmune attack on the thyroid gland known as Hashimoto’s thyroiditis, a condition that has 5 progressive stages. [Read the 5 Stages of Hashimoto’s]
This autoimmune attack starts with thyroid antibodies, that lead to an attack, and eventual destruction of the thyroid gland until it is no longer able to make thyroid hormone. These antibodies can be tested in the blood, however, the patients in the NEJM study were not tested for the antibodies. Antibodies can be present for decades before a change of TSH is seen.
Subclinical hypothyroidism is the third stage of the condition, while overt hypothyroidism is the 4th. When the TSH is between 2.5 and 10 μIU/mL and T3 and T4 is within normal limits, this is known as subclinical hypothyroidism (at this point, people may or may not have thyroid antibodies). This means that your thyroid is still able to make enough thyroid hormone, but not without sacrifice. At this point, our thyroid is working overtime, and this often leaves us with thyroid symptoms like fatigue, hair loss, and cold intolerance.
The thyroid is constantly getting a signal to make more and more hormone, and your body is likely running out of nutrients (like selenium) to make more hormone. This results in additional inflammation of the thyroid, attracting more antibodies and fueling the autoimmune process. As many as 5% of people with subclinical hypothyroidism will progress to overt hypothyroidism each year.
Korzeniowska and Colleagues at the Medical University of Gdansk found that treating children with subclinical hypothyroidism with thyroid hormones resulted in a decrease of inflammation. This means that the medications gave their thyroids a rest and resulted in a slowing down of the autoimmune attack manifested by lower levels of thyroid antibodies. (1)
The Impact of This New Study
I am concerned that as a result of this study, many people will not receive the care that they deserve. In this day and age, it takes an educated patient to get proper care.
If you are taking levothyroxine and are struggling with thyroid symptoms, please educate yourself. Do not let your doctor, or a poorly designed study, stand in the way of you feeling better.
First Step: Get to Know Thyroid Symptoms
Symptoms that suggest hypothyroidism or under treatment with thyroid hormones include:
- Tangled hair
- Eyebrow thinning/loss
- Puffy face
- Brain Fog
- Sadness/apathy
- Fatigue
- Cold intolerance
- Weight gain
- Joint pain
- Heavy periods
Symptoms that indicate hyperthyroidism or overtreatment with thyroid hormones include:
- Hair Loss
- Irritability
- Agitation
- Mood swings
- Restlessness
- Palpitations
- Heat intolerance
- Rapid heart rate
- Scant periods
- Weight loss
- Insomnia
- Excess sweating
Second Step: Educate Yourself!
I’ve decided to release my Optimizing Thyroid Medications eBook, a special bonus for my new book Hashimoto’s Protocol, to everyone as a free download. This eBook has all of the information you need to be an empowered patient to ensure that your thyroid hormones are optimized properly so that you can feel your best!
Download your copy of Optimizing Thyroid Medications below!
Third Step: Get Your Thyroid Tested
Start by getting your thyroid function tested — I wrote a blog post on the 10 most important thyroid tests. Be sure to get a copy of your own lab results to ensure that you are getting the proper care.
Fourth Step: Use Your Empowered Voice to Advocate for Yourself to Receive Proper Care
If you have a doctor that won’t give you the proper care, find a different doctor. My readers have been submitting names of helpful doctors for quite some time now 🙂
References
- Katarzyna K, Jarosz C, Agnieszka S et al. L-thyroxine Stabilizes Autoimmune Inflammatory Process in Euthyroid Nongoitrous Children with Hashimoto’s Thyroiditis and Type 1 Diabetes Mellitus. Journal of Clinical Research in Pediatric Endocrinology. 2013;5(4):240-244. doi:10.4274/jcrpe.1136.
2. Span P. Could Be the Thyroid; Could Be Ennui. Either Way, the Drug Isn’t Helping. Nytimescom. 2017. Available at: https://www.nytimes.com/2017/04/21/health/could-be-the-thyroid-could-be-ennui-either-way-the-drug-isnt-helping.html. Accessed August 8, 2017.
3. Stott D, Rodondi N, Kearney P et al. Thyroid Hormone Therapy for Older Adults with Subclinical Hypothyroidism. New England Journal of Medicine. 2017;376(26):2534-2544. doi:10.1056/nejmoa1603825.
4. Wiersinga W. Paradigm shifts in thyroid hormone replacement therapies for hypothyroidism. Nature Reviews Endocrinology. 2014;10(3):164-174. doi:10.1038/nrendo.2013.258.

Hello Dr. Izabella.
I am a 53 year old with diabetes, no thyroid (complete thyroidectomy in Sept 2009 due to a precancerous nodule and 11 other ones) and problems with low normal (not optimal) iron levels. I live in Australia and didn’t know then what I know now about the thyroid and nodules. I had a perfectly functioning thyroid (TSH on day before surgery was 0.1) I was also very blessed in 2010 to find a specialist GP that took me off my almost 200mcg dose of thyroxine (I’m only 5’5″ and average wt although that is getting worse lately) and put me on T3/T4 natural thyroid meds. What a difference! However, lately I’m gaining weight, have a leaky gut and my iron levels have ranged from 36 to 91 after iron injections, but back to 71. My doctor wants the levels to be at 100 so I’m on another round of injections. Which leads me to the reason I’m writing.
Today I got my third injection with a local GP (between work and the location of my prescribing doctor it isn’t easy for me to get in to see him, so I went to a local clinic). And for the second time in a week I have been talked down to and been told flat out that my iron levels are fine and they would not advise an injection. I hear you speak of this attitude amongst GP’s, but had not actually encountered it until last week and today. I chose to go to this clinic as it is close to home, and it turns out the nurse is very good at giving the injection. However last week a different doctor also told me she wasn’t happy about allowing the nurse to give it to me, but since I was there she would allow it. However she flatly told me she would not see me again. So I asked to see a different doctor in the clinic. And today, got the same response. And today I got charged significantly more! I guess I have been very blessed to have found 2 other doctors who treat my thyroid and diabetes, who actually listen to me….my current specialist GP asks me what I want to do at my quarterly appointments. But this iron level issue has been so frustrating. Do you have any more information as to why I can’t seem to maintain an optimal level? Is the gut the key? I’m not technically Hashimoto’s (don’t have the antibodies), but I definintely have all the symptoms of being hypothyroid despite taking T3/T4.
I want to give these 2 doctors a copy of your ferritin report, but am pretty much convinced that they are too arrogant to even read it. I tried to give the doctor today a bit of history of me, but she really wasn’t interested except to send me to a specialist…a haematologist. I know my iron levels are related to my thyroid, but I’m not a doctor and she only listens to specialist doctors. I have a doctor who prescribed the injections, but they don’t accept what another doctor with a different methodology and ideology has prescribed. How rude is that? So for the first time I felt so angry and frustrated….what you and so many of the people on the Thyroid Secret said of their experiences with medical doctors!
So, I want to thank you for all you do to provide those of us who aren’t doctors, but who want to be able to understand what is going on in our own bodies, with the information and knowledge to be able to find good doctors and ask for the right tests and medications. I just wish that I had known all this before my thyroidectomy!!!! I’m pretty sure my nodules could have been reduced if I’d known what to do…I think I was/am probably estrogen dominant. My sister had stage 1 estrogen receptor breast cancer, and last year developed a nodule in her thyroid. She only had half of it removed and I think my knowledge was helpful when she spoke to her doctors about the surgery and tests, and establishing baseline values. I am always learning more and more.
Blessings to you.
BTW I bought the Thyroid Secret, but haven’t gotten your books as I wasn’t sure if I should…since I’m not Hashimotos. What do you suggest? Get the Protocol book? Thanks again.
Naomi
Naomi – thank you for following this page and for your support. <3 I'm sorry to hear that you had such a disappointing experience. 🙁
You may be interested in my 12 week online program called Hacking Hashimoto’s that covers all of the strategies that I go through with my one-on-one clients, in a self-paced format, so that participants have access to all of the things I’ve learned about Hashimoto’s without having to schedule costly consults with me or another practitioner. There are a few requirements that you should pay attention to, such as my book is a required read.
HACKING HASHIMOTOS
http://hackinghashimotos.com/
In addition, any person that goes through the program will have the opportunity for a follow up consultation with one of my thyroid pharmacist consulting members.
Diabetes/cancer/low minerals can be due to gluten. Gluten may lower the immune/hurt intestines so less minerals like iron absorb or less a person bleed that causes loss of iron. Low iodine may cause cysts. Cancer may happen at premenopause when progesterone is lowering and at menopause when progesterone stops which helps the immune system/thyroid/blood sugar/energy. Estrogen dominance maybe due to meat/dairy/soy/BPA/fat/chemicals/The Pill which may block thyroid and promotes cancer. Taking Bioidentical hormones may help. Gluten may hurt all glands…liver/pancreas/thyroid/pituitary etc… Detoxing may help the thyroid/chemical reactions work better. Far Infrared Sauna may help. Hair tests show good minerals/heavy metal levels.
You rock!!
Thanks for setting them straight!!!
Thank you for standing up and being a voice of reason and common sense. Life is sweet and easy to live when the “other” voices aren’t listened to.
Jill – thank you for following this page and your kind words! <3
I am really hoping to build a database of testimonials to submit to a medical journal. I would very much love if you submitted your story. You would be helping so many. Would you consider doing this?
http://www.thyroidpharmacist.com/testimonial
I love you so much for this one and the thing is. I’m so happy now that I’ve found this one I need your help Thank you so much Linda Bledsoe
Linda – thank you for following this page and for referring. Do you have Hashimoto’s or a thyroid condition?
Hashimoto’s is a complicated condition with many layers that need to be unraveled. While conventional medicine only looks at each body system as a separate category and is only concerned with the thyroid’s ability to produce thyroid hormone, Hashimoto’s is more than just hypothyroidism. I wanted to pass along these articles that I wrote. I hope they help 🙂
WHERE DO I START WITH HASHIMOTO’S
https://thyroidpharmacist.com/articles/where-do-i-start-with-hashimotos/
OVERCOMING HASHIMOTO’S
https://thyroidpharmacist.com/articles/overcoming-hashimotos-in-the-new-year
Hello,
First, thank you so much for the webinar you recently completed. Fantastic! You put everything you had into this. The information was invaluable. Plan on purchasing your book. My son has been diagnosed with Hashimoto’s. Also, my thyroid tests appear to be within normal ranges, but have low morning temperature of 96.9-97.4. Is that considered low and possibly come under subclinical thyroid? I have had issues with fatigue and trouble losing weight since having epstein-barr.
Thank you so much for giving your time, care and passion in this area.
Brenda – thank you for following this page and for your support. <3
I highly recommend that you work with a functional medicine clinician. It’s a whole medical specialty dedicated to finding and treating underlying causes and prevention of serious chronic disease rather than disease symptoms.
FUNCTIONAL MEDICINE APPROACH TO THE THYROID
https://thyroidpharmacist.com/articles/functional-medicine-approach-to-the-thyroid
WHAT TYPE OF DOCTOR SHOULD YOU SEE IF YOU HAVE HASHIMOTO’S
https://thyroidpharmacist.com/articles/what-type-of-doctor-should-you-see-if-you-have-hashimotos
10 THINGS I WISH MY ENDOCRINOLOGIST WOULD HAVE TOLD ME
https://thyroidpharmacist.com/articles/10-things-i-wish-my-endocrinologist-would-have-told-me
CLINICIAN DATABASE
http://www.thyroidpharmacistconsulting.com/clinician-database.html
FIND A FUNCTIONAL MEDICINE CLINICIAN
https://www.functionalmedicine.org/practitioner_search.aspx?id=117
Hi – I have been following your facebook & my question is :
I have been tested – I was on 25 – 50 – now 75 synthroid
My test results are :
TSH (f) 8.12. (Was 9.57 on the 50mg)
My free T4-T4 free. Is 11.6
What suggestions/advice do you recommend. – if you can?
Thanks – Lynn
Lynn – thank you for following this page. Please, understand that due to liability issues, I am unable to answer specific medical questions.
I highly recommend that you work with a functional medicine clinician. It’s a whole medical specialty dedicated to finding and treating underlying causes and prevention of serious chronic disease rather than disease symptoms.
FUNCTIONAL MEDICINE APPROACH TO THE THYROID
https://thyroidpharmacist.com/articles/functional-medicine-approach-to-the-thyroid
WHAT TYPE OF DOCTOR SHOULD YOU SEE IF YOU HAVE HASHIMOTO’S
https://thyroidpharmacist.com/articles/what-type-of-doctor-should-you-see-if-you-have-hashimotos
10 THINGS I WISH MY ENDOCRINOLOGIST WOULD HAVE TOLD ME
https://thyroidpharmacist.com/articles/10-things-i-wish-my-endocrinologist-would-have-told-me
CLINICIAN DATABASE
http://www.thyroidpharmacistconsulting.com/clinician-database.html
FIND A FUNCTIONAL MEDICINE CLINICIAN
https://www.functionalmedicine.org/practitioner_search.aspx?id=117
Just had an endo appointment, and even though levels are all good, I still suffer insomnia, hair loss, and I cannot take any heat over 70 degrees. What can I do to get my thermostsat reset?
Kathy – thank you for following this page.
The thyroid gland has been called a thermostat for our body, as it helps to regulate heat. People with hypothyroidism are prone to having low body temperatures and cold intolerance. It’s one of those symptoms that we often brush off, don’t notice and don’t take seriously, but can be very distressful when we do not take the proper precautions. Here’s an article that I hope helps you.
THYROID AND COLD INTOLERANCE
https://thyroidpharmacist.com/articles/thyroid-and-cold-intolerance
Hi, does your book or books comes in spanish? Thanks
Maria – thank you for following this page. Yes, we are working on translating it into different languages.:)
Well said Izabella! So glad to have some like you on our side advocating for us and educating people. We love you!
1. Thank-you for all your work, dedication and passion in bringing these data to the “masses.”
2. I would like to suggest that the TRH stimulation test be used in diagnosing thyroid issues, along with the use of thyroid ultrasound.
3. Following anesthesia induced brain injury with debilitating cascading effects, I developed a number of auto immune disorders: CFIDS, fibromyalgia, Hashimoto’s thyroiditis, endometriosis, uterine fibroids. Being brought up in the natural health tradition, I went to naturopaths, chiropractors, oriental medicine practitioners, massage therapists, etc. I also expanded my “search” to include DOs and MDs. What I have found is that many well-meaning clinicians of whatever ilk practice their own form of “orthodox medicine” and blame the patient when their particular protocol does not work. It took years before I was diagnosed with thyroiditis. I am convinced that a TRH stimulation test or thyroid ultrasound might have found the disorder much more quickly.
4. Having a CFIDS diagnosis is a complication, and I guarantee you that people who have not experienced this form of malaise have absolutely no concept of how debilitating it can be, anymore than people, including family, understand severe thyroid problems. I am absolutely not surprised that subclinical hypothyroidism (which I am convinced is simply, not to mention, egregiously under/undiagnosed because of improper testing) is viewed with severe skepticism. After all, who is mostly effected? Women. Just know that most any problem a woman has, really will be assumed to be “all in the head” and that we are lazy, attention mongers; suffering from emotional issues, not the least of which is ennui. What I truly find sad, is that the “problem” truly is a whole body issue and surprisingly! this does include the head/brain. People in the CFIDS/ME /fibro community (mostly women) have suffered extreme prejudice and sadly, constantly battle this form of emotional/mental abuse.
5. Let’s not let this injustice continue. Let’s get doctors trained in differential diagnostic testing. Let’s hold the “supervisory” medical associations/insurance companies accountable for their unfeeling, uncaring usurping of patients’ rights whilst promulgating insane dictums of “standard of care” doctors are required to follow.
6. Let’s put an end to the emotional/mental abuse. And might I add, this is also physical abuse; non treatment because of improper diagnostics is most assuredly potent and potentially lethal physical abuse. Let’s stop this physical abuse as well.
Andrée – thank you for following this page and for sharing.
I highly recommend that you work with a functional medicine clinician. It’s a whole medical specialty dedicated to finding and treating underlying causes and prevention of serious chronic disease rather than disease symptoms.
FUNCTIONAL MEDICINE APPROACH TO THE THYROID
https://thyroidpharmacist.com/articles/functional-medicine-approach-to-the-thyroid
WHAT TYPE OF DOCTOR SHOULD YOU SEE IF YOU HAVE HASHIMOTO’S
https://thyroidpharmacist.com/articles/what-type-of-doctor-should-you-see-if-you-have-hashimotos
10 THINGS I WISH MY ENDOCRINOLOGIST WOULD HAVE TOLD ME
https://thyroidpharmacist.com/articles/10-things-i-wish-my-endocrinologist-would-have-told-me
CLINICIAN DATABASE
http://www.thyroidpharmacistconsulting.com/clinician-database.html
FIND A FUNCTIONAL MEDICINE CLINICIAN
https://www.functionalmedicine.org/practitioner_search.aspx?id=117
Hi Dr. Wentz,
Thanks for the great article. I have a son (20 years old), who deals with so many hypo symptoms, but is always very warm. He has had thorough blood tests and his antibodies are normal. His tsh in Oct ’15 was 4.71, Dec ’16 was 6.29 and in Feb ’17 was 2.95. He was also diagnosed with Supraventriculat Tachycardia during this time period with heart rates as high as 260 bpm for extended periods, requiring E.R. visits. The doctors are pushing for a cardiac ablation, but I have a strong feeling this is thyroid related. His primary did prescribe an extremely low dose of bioidentical t3 1 mcg/ t4 25 mcg SR, but the palpitations got worse, so he had to discontinue. In your opinion, should I push for a thyroid ultrasound or do you think the tachycardia is unrelated?
I would appreciate a little guidance, as I am the only one in my family that believes the tachycardia is being caused by something other than an “extra electrical pathway” in his heart.
Thank you so much for all you do to educate us!
Marie
Marie – thank you for following this page. My heart goes out to you and your son! <3
Here are the tests you need for diagnosis. Most endocrinologists don't run them all so you will have to request them. Make sure to request a copy of your labs as well.
TOP 6 THYROID TESTS
https://thyroidpharmacist.com/articles/top-6-thyroid-tests
You may also like to check out the doctors that other patients recommend on this list:
CLINICIAN DATABASE
http://www.thyroidpharmacistconsulting.com/clinician-database.html
FIND A FUNCTIONAL MEDICINE CLINICIAN
https://www.functionalmedicine.org/practitioner_search.aspx?id=117
I’m from Italy and i’ m learning a lot from this website as a patient! Thanks!
I would like to address you to this interesting and recent article that confirm all your precious advices for Hashimoto’patients:
https://www.ncbi.nlm.nih.gov/pubmed/28315909
Thanks again
Bibbio – thank you for following this page and for sharing! 🙂
Last year physical showed 5.530 u[IU]/mL. This years showed 12.140 u[IU]/mL. About a week later did a blood test again that showed 8.870 u[IU]/mL. My T4 was the only other thing besides tsh that got tested and it was normal.
I’m so tired. Sometimes so much that I feel I could close my eyes for a moment and be out. My hair is thinning, I usually have really thick hair all over and my hair stylist wven noticed saying is was way thinner on bottom compared to top, but alot of hair comes out when washing and brushing, more than she feels normal. My cold intolerance is very low. My toes and fingers feel like ice sometimes. What do I do?
Natasia – thank you for reaching out. My heart goes out to you. <3 Please understand, I am not able to respond directly to these types of questions here. I highly recommend that you work with a functional medicine clinician. It’s an entire medical specialty dedicated to finding and treating underlying causes and prevention of serious chronic disease rather than disease symptoms.
FUNCTIONAL MEDICINE APPROACH TO THE THYROID
https://thyroidpharmacist.com/articles/functional-medicine-approach-to-the-thyroid
CLINICIAN DATABASE
http://www.thyroidpharmacistconsulting.com/clinician-database.html
FIND A FUNCTIONAL MEDICINE CLINICIAN
https://www.functionalmedicine.org/practitioner_search.aspx?id=117
Hi Dr. Wentz,
Thanks for the great article.
I m 40 years old.
My TSH level was
14 Feb, 18 = 19.98
20 Feb, 18 = 18.26
22 Feb, 18 = 21.70
My question is what are the possible reasons of high levels of TSH and now what I can do next?
Thanks
Khurram – Thank you for following this page. Most people feel best with a TSH of around 1 or lower and with a Free T4 and Free T3 in the upper half of the range. It is expected that your TSH will be very suppressed when optimal on NDT medication. How much thyroid replacement therapy is needed is unique and different for each person, so it’s important to work with a functional medicine practitioner or a doctor, who can closely monitor your dosage and your progress.Every six weeks is usually a good schedule for testing your thyroid hormones.
These are the recommended thyroid function tests from page 32 of my book:
– TSH
¨ TPO Antibodies
¨ Thyroglobulin Antibodies
¨ Free T4
¨ Free T3
¨ Reverse T3 (optional)
¨ Thyroid Ultrasound (optional)
Here is a research article which might help further:
TOP 10 THYROID TESTS FOR DIAGNOSIS
https://thyroidpharmacist.com/articles/top-6-thyroid-tests/
I’m a 59 year old woman dealing with Hashimoto/ Hypothyroidism since 2006. I have been to internist and endocrinologist and it’s been very difficult to manage my levels. My TSH level would show I would be in a hyper state currently off the chart so the endocrinologist have been medicating me with both Armour and Synthroid managing my T3 and T4 levels which are within range. I don’t have symptoms of hyperthyroidism in fact I am so fatigue I can hardly get through dishes and laundry. I’ve checked my blood pressure which is very low and pulse. There is so much information on the web I don’t know what direction to turn in. This endocrinologist has changed my medication 6 times this year and I’ve gained 20 pounds. I had eliminated gluten, dairy,soy,corn,eggs,canola oil, pork for 30 days and I only lost 1 pound. Can Armour skew your TSH levels? What’s causing this havoc? What medications can I ask my endocrinologist about? I just want to feel good again. I spend days in bed these days. So wish I could consult you.
Desperate seeking assistance.
Diane – thank you for following this page. We know that intestinal permeability (aka leaky gut) is present in every case of autoimmunity and often precedes the development of Hashimoto’s. Symptoms of leaky gut may include bloating, diarrhea, constipation, stomach aches, acid reflux and irritable bowel syndrome. According to the Institute of Functional Medicine, many people develop IBS 5-10 years before an autoimmune diagnosis. I was one of them and didn’t take my gut health as seriously as I should have. Gut problems are often caused by infections like H. pylori, parasites like Blasto, SIBO, an imbalance of bacteria, and enzyme deficiencies or food sensitivities (especially to gluten, dairy, and/or soy). Even stress can be a factor in gut permeability. You might be interested in our Root Cause Reset detox program that we are offering for the first time and for a limited time only. Check it out!
https://thyroidpharmacist.com/enroll-in-root-cause-reset/
My TSH is of 6.3, the rest is normal. I don’t have symptoms (or vary vague). I refused treatment because I have always heard that, with no symptoms and a TSH under 10, it is better not to take meds, seeing that many people (with no symptoms) start to developping them after starting treatment. It is not yet clear whether this situation needs meds or not. I prefer not to take them. I am trying a gluten/dairy-free diet to see if TSH lowers.
Silvia – thank you for sharing! I’m looking forward to seeing your progress here. Here is an article you might find interesting as well.
THE 5 STAGES OF HASHIMOTO’S THYROIDITIS
https://thyroidpharmacist.com/articles/5-stages-hashimotos-thyroiditis/
Why my endocrinologist never changed my antithyroid medication dose even my thyroid level up and down freet3 up TSH was 0.01 this is I believe wrong and ignorant specialist my dose was 300 mg PTU almost 8-9 years this is crazy sometimes my TSH was normal but I was still taken PTU 300 mg
Tekin – thank you for reaching out. Most people feel best with a TSH of around 1 or lower and with a Free T4 and Free T3 in the upper half of the range. It is expected that your TSH will be very suppressed when optimal on NDT medication. How much thyroid replacement therapy is needed is unique and different for each person, so it’s important to work with a functional medicine practitioner or a doctor, who can closely monitor your dosage and your progress. Every six weeks is usually a good schedule for testing your thyroid hormones. I highly recommend that you work with a functional medicine clinician. It’s an entire medical specialty dedicated to finding and treating underlying causes and prevention of serious chronic diseases, rather than disease symptoms. If you cannot find a Functional Medicine practitioner in your area, it is possible to work with an overseas practitioner remotely via Skype or some other online video platform. Here’s a link which might help: https://thyroidpharmacist.com/database-recommended-clinicians/
Here is a research article which might help further as well:
TOP 10 THYROID TESTS FOR DIAGNOSIS
https://thyroidpharmacist.com/articles/top-6-thyroid-tests/
Hello Dr Izabella,
Thank you so much for your books and your website! I just ordered all of them via amazon.
Do you or anyone happen to know a good doctor in the south of Germany? I most likely have stage 2 or 3 Hashimotos but I can´t find a doctor who sees it. They all say even despite my antibodies, my TSH is fine, so I am fine.
I also have inflammatory PCOS with high androgens. My TSH was 2,3 and my TPO were 31. I have all the symptoms like heavy periods, hair loss, extreme fatigue ( I could sleep 24 hours if nobody would wake me up), leg aches (honestly the worst, I can´t even go and take a walk with my boyfriend) etc.
So much love and appreciation for all of you,
Jenny
Jenny – you are very welcome! ❤️ I’m so sorry you are struggling with all of this. My heart goes out to you. I believe that everyone needs to find a practitioner that will let them be a part of the healthcare team. You want someone that can guide you, that will also listen to you and your concerns. You want someone that’s open to thinking outside of the box and who understands that you may not fit in with the standard of care. It’s a good idea to ask some standard questions when contacting a new doctor for the first time. Something else to consider is you can work with a functional doctor remotely, via Skype. You could also contact your local pharmacist or compounding pharmacy, who may be able to point you to a local doctor who has a natural functional approach. But I encourage you to keep looking for the right one for you! Here are some resources you might find helpful.
CLINICIAN DATABASE
https://thyroidpharmacist.com/database-recommended-clinicians/
FIND A FUNCTIONAL MEDICINE CLINICIAN
https://ifm.org/find-a-practitioner/
COMPOUNDING PHARMACIES
https://thyroidpharmacist.com/database-recommended-compounding-pharmacies/
is there an article or do you have any thoughts on subclinical hypothyroid with symptoms of hypothyroid as well as hyperthyroid symptoms such as high appetite with no weight gain and scant period? I have encountered this a few times.
Sarah – thank you for reaching out. People with Hashimoto’s may experience BOTH hypothyroid and hyperthyroid symptoms because as the thyroid cells are destroyed, stored hormones are released into the circulation causing a toxic level of thyroid hormone in the body, also known as thyrotoxicosis or Hashitoxicosis. Eventually, the stored thyroid may become depleted and due to thyroid cell damage, the person is no longer able to produce enough hormones. At this time, hypothyroidism develops.
THE MANY FACES OF HASHIMOTO’S
https://thyroidpharmacist.com/articles/the-many-faces-of-hashimotos/
10 FACTS ABOUT THYROID DISEASE
https://thyroidpharmacist.com/articles/need-know-thyroid-disease/
GRAVES AND HASHIMOTO’S
https://thyroidpharmacist.com/articles/graves-vs-hashimotos/
Great information! I’m really struggling (in the Netherlands) how to treat or not treat subclinical hypothyroidism. Regular endocrinologist in academic hospital says that my lab values are perfectly fine despite the fact i have all the hypothyroid symptoms, literally every box I can tick just not the overweight symptom as I eat very healthy and do all the things you mention in your books. Despite it all my lab values and symptoms stay the same. TSH 3.7, free t4 11.8 and free t3 3.6.
My t4 levels are below the reference but TSH and free t3 are within reference range.
Then what to do if no other cause or deficiency has been found ( only low ferritin levels) and I have all the hypothyroid symptoms and can’t seem to function as a normal healthy women age 40? No perimenopause, no low progesteron etc just the subclinical thyroid and symptoms?
Isn’t it worth a try to see if a little bit of levothyroxine would help or is it very risky and I just have to live with chronic fatigue and symptoms for the rest of my life?
Lucyna – I hear your frustration, it can feel so discouraging to have classic hypothyroid symptoms while your lab results appear “normal” by standard reference ranges. In my protocols and research, we recognize that some people with subclinical hypothyroidism or lab values in the upper-normal TSH range can still experience significant symptoms. Addressing this usually starts with a comprehensive approach: supporting nutrient status (like your ferritin), gut health, adrenal function, and addressing any other underlying contributors to symptoms. If your doctor will not prescribe the medication you are looking for, you may consider asking your local pharmacist for doctors in your area who prescribe the medication you are looking to try. I’m a big fan of using everything we can to get ourselves better.